 Yesterday we discussed a case of hemoptysis NYD and today we reviewed an elderly gentleman with acute renal failure who was diagnosed with Goodpasture's syndrome.
Yesterday we discussed a case of hemoptysis NYD and today we reviewed an elderly gentleman with acute renal failure who was diagnosed with Goodpasture's syndrome.Yesterday's differential diagnosis for hemopytsis included vasculitis. In particular one always needs to consider pulmonary-renal syndromes in the differential for hemoptysis, including Wegener's Granulomatosis (WG) and Goodpasture's syndrome.
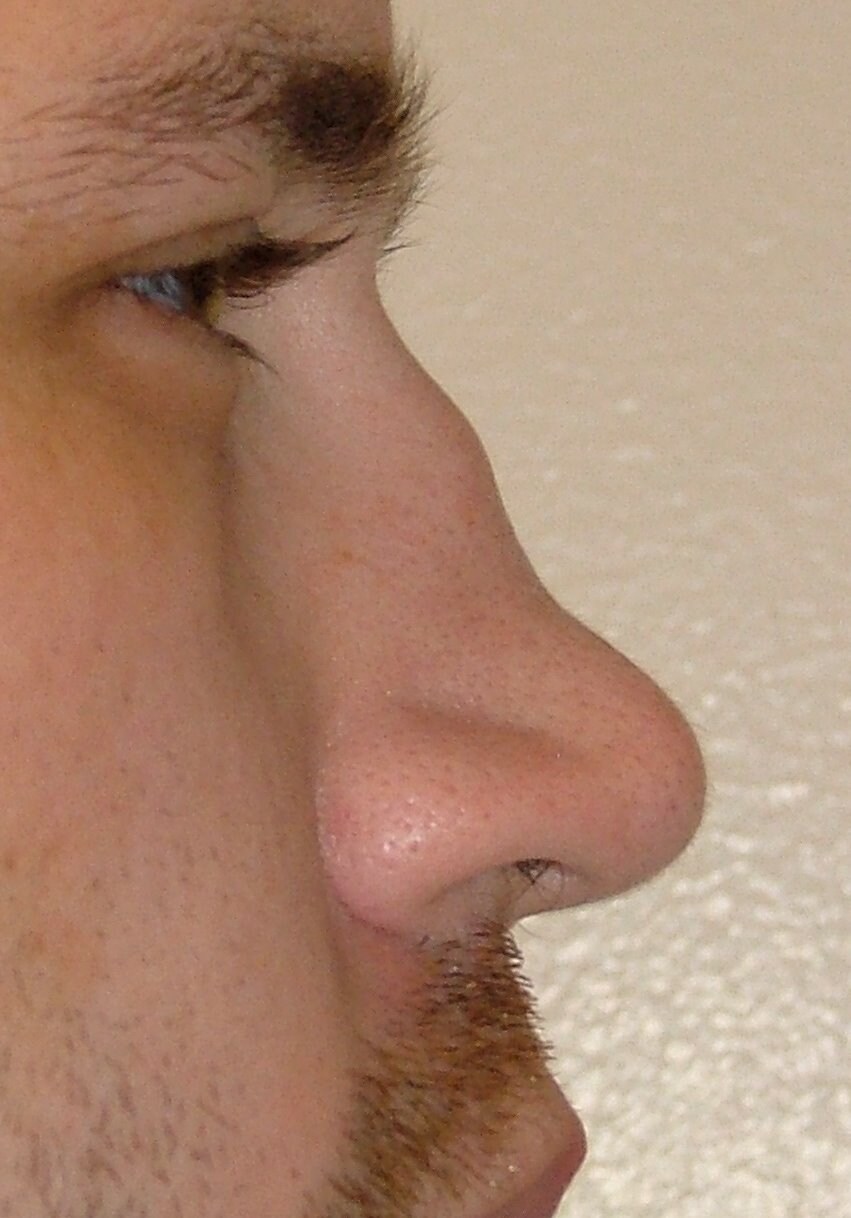
WG's can present in many ways, but often involves a history or sinusitis or rhinitis, along with constitutional symptoms, hemoptysis, renal failure, and occassionally polyarthralgias. Patients can develop a "saddle nose" due to collapse of their nasal support.
{kind=link}
The pathological triad of WG includes:
1) systemic necrotizing angiitis
2) necrotizing granulomatous inflammation of the respiratory tract
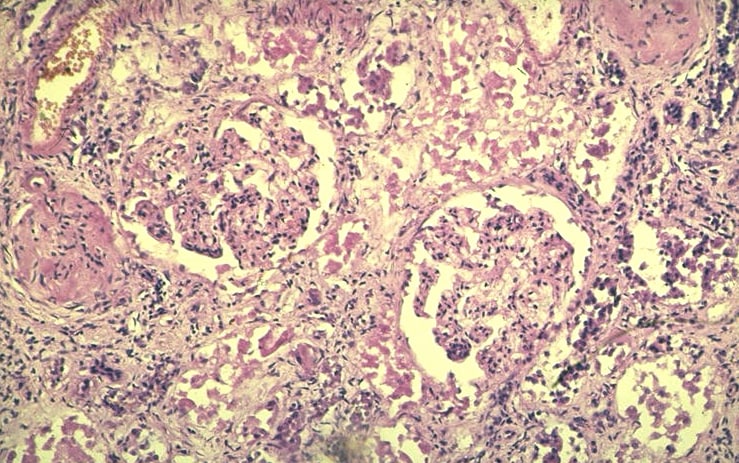
3) necrotizing glomerulonephritis
Diagnosing Wegener's requires a detailed history and physical exam as well as blood work, looking for evidence of c-ANCA or anti-PR3, a urinalysis looking for RBC casts, chest imaging, and often a biopsy of either the kidney or lung. Lung biopsies frequently reveal evidence of vasculitis and granulomatous inflammation. Renal biopsies demonstrate a Pauci Immune picture (i.e.: no deposition of immunoglobulin or complement) with segmental crescentic necrotizing glomerulonephritis.
{kind=link}
{kind=link}
Treatment includes pulsed steroids and often cyclophosphamide urgently as this is a rapidly progressive disease. Involvement of a rheumatologist and nephrologist for management and follow-up is usually warranted.
Goodpasture's disease is a triad of pulmonary hemorrhage, glomerulonephritis (GN), and circulating anti-glomerular basement membrane (anti-GBM) antibodies in the blood. However, not all patients present with the triad, but anti-GBM antibodies is a distinguishing feature of Goodpasture's. Most patients (~60 - 80%) present with both pulmonary and renal disease, 20 -40% have only renal disease, and less than 10% have only pulmonary disease.
Diagnosis, like WG, involves a thorough history and physical exam as well as blood work looking for anti-GBM antibodies, chest imaging, and usually a renal or lung biopsy. Direct immunofluorescence of the renal biopsy will light up and stain along the basement membrane, reflecting the deposition of IgG.
{kind=link}
Treatment again, requires rapid aggressive management; however, in the setting of Goodpasture's there is a role for plasmapheresis to remove any circulating anti-GBM antibodies. This occurs in conjunction with immunosuppression with pulsed steroids and often cyclophosphamide. Again, consultation with a nephrologist is often warranted!
Here is a review on the differential diagnosis of hemoptysis and here is a brief case report and review of Goodpasture's from The Lancet.
Am Abdul Hakim so joyful giving this testimony of genius herbalist,Dr Moses anabic herbal home whom cured me of liver cancer.i was diagnosed of liver cancer 2years back I tried to cope with the sickness but unfortunately it had gone so bad,I went to so many medical centres I was told to go for a special xray which was computed tomography scan.it's result came out that my liver was rottening and was told that there was no cure,I collapsed there at the centre after getting myself an individual who came for a test after being cured from hiv,then gave me an email address of dr Moses anabic so I contacted him and he assured me of a total cure after three weeks of administering his herbs and I was cured totally.nothing is impossible for God almighty any individual suffering from any illness or virus no matter how bad it may be,don't ever think it's impossible.contact him through his personal email address via MOSESANABIC@GMAIL.COM or write him on WhatsApp with +2348100661264.thank you very much doctor Moses.
ReplyDelete