
Malaria - What's up with that?
Malaria is caused by the protozoan Plasmodium. The mosquito that carries Plasmodium species called Anopheles (literally translated to 'ueseless'). Due to their transmission of malaria, mosquitos are thought to have caused half of all human deaths - more than all the wars combined.
Malaria should be suspected in anyone with a fever that has had mosquito exposure in a region where malaria is endemic. Don't expect to get a history of 'mosquito bites' from patients, just assume that they got mosquito bites when they traveled in the area. The incubation period for malaria: can range from 2 weeks (often falciparum) to a year, due to potential latency of the organisms. The diagnosis of malaria is based on light microscopy of thick and thin smears of patient blood - which are highly sensitive for detection of parasites when the load is >1%. When the parasite load is low, antigen testing is able to detect infection, though antigen testing cannot reveal the quantity of organisms infecting a patient. Also, it may or not be able to differentiate falciparum species from non-falciparum species.

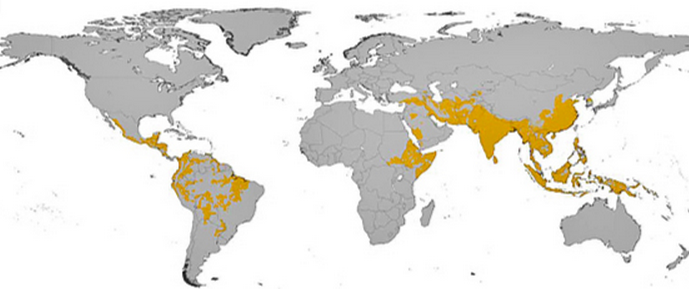
The top map shows falciparum distribution and the bottom shows vivax distribution.
4 Malaria Questions to consider for treatment in a patient diagnosed with Malaria:
1) Is this uncomplicated or complicated malaria?
2) Where it was acquired, and what are the resistance patterns there?
3) What species of malaria is it?
4) What is the degree of parasitemia?
1) Presentation of Malaria: Signs vs Symptoms
Uncomplicated vs Complicated Presentation of Malaria
In general, patients who are not obtunded and can take PO medications are considered "uncomplicated".
Uncomplicated Malaria - Usually presents with non-specific symptoms, such as chills, fatigue, diaphoresis, headache, nausea/vomiting, abdominal pain, diarrhea, arthralgias, and myalgias
On physical examination, the most prominent and common findings are splenomegaly and jaundice. This may be found even in patients without complicated malaria. Common lab abnormalities in patients with uncomplicated malaria include thrombocytopenia (very common) and anemia. Elevated liver enzymes, elevated creatinine, and raised WBC are also seen.
Complicated Malaria
- Altered consciousness +/- seizures
- Respiratory distress or acute respiratory distress syndrome (ARDS)
- Circulatory collapse (shock)
- Metabolic acidosis
- Renal failure, hemoglobinuria ("blackwater fever")
- Liver failure
- Coagulopathy with or without disseminated intravascular coagulation
- Severe anemia or massive intravascular hemolysis
- Hypoglycemia
2) Location of Acquisition
Location of acquisition is relevant to understanding whether the organism is expected to be resistant or not. When in doubt, treat all falciparum organisms as if they are resistant to chloroquine. Chloroquine sensitive areas include Central America, Haiti, the Dominican Republic, former Soviet Union nations, and most of the Middle East. Anywhere outside of these regions is considered to be chloroquine resistant. Potential areas of resistance to artesunate include southeast Asia (especially Cambodia).

3) Species of Malaria
- Non-falciparum (P. vivax, P. ovale, P. malariae, P. knowlesi) cause febrile illnesses but are rarely fatal.
- However, P. falciparum infections are more virulent and can rapidly progress to fatal illness.
- It is often impossible to determine the species of malaria infection on clinical grounds alone. This can be established through antigen testing and can sometimes be established based on the location of acquisition
4) Level of Parasitemia
This refers to the percentage of RBCs carrying the organism and is established by examining the blood smear. In uncomplicated malaria, loads tend to be >5% in low transmission areas and 10% in high transmission areas.

Treatment
With chloroquine sensitive strains (determined by location of acquisition), the first line of therapy is either hydroxycloroquine or chloroquine. Side effects of these medications include GI upset, retinopathy, and pruritus.
With chloroquine resistant strains, first line therapy usually includes Artesunate based therapy or Atovaquone-based therapy (+proguanil). Artesunate therapy is generally very well tolerated.
What's that picture of the top? That's the building of the Panama Canal, 1904-1914. Malaria and yellow fever were rampant during the construction. Overall, 5600 people died building the canal.
An excellent resource for malaria, as indicated by Dr. Paul Bunce:
nice article.i like it.thanks.
ReplyDeleteVitamin b17 in Cancer