Today we discussed the diagnosis and management of a pulmonary embolism (PE) and the role of Inferior Vena Cava (IVC) filters.
The role of IVC filters in PE remains controversial and there is significant variability in clinical practice. Guidelines from the ACCP exist, however recent evidence suggests that up 25% of IVC filter insertions are done for indications that do not follow the guidelines.
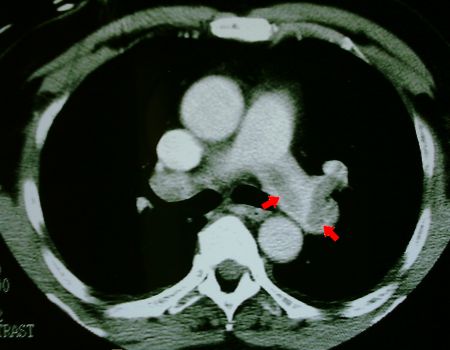
As mentioned today, IVC filters can be associated with catastrophic consequences in the event of filter fracture and embolism as discussed in this 2010 study.
Here's an excellent recent review on acute PE from the NEJM this year and a link to the PIOPED II Trial we discussed today.
A few points on the diagnosis and management of a PE with a focus on IVC filters:
1) The diagnosis or exclusion of a PE is heavily influenced by the pre-test probability before objective testing begins. The Well's criteria is a well validated scoring system to estimate the pre-test probability of a PE:
i) Clinical symptoms of a DVT - (3 points)
ii) Other dx less likely than PE - (3 points)
iii) HR greater than 100 - (1.5 points)
iv) Immobilization for more than 3 days or
surgery within the past 4 weeks - (1.5 points)
v) Previous DVT/PE - (1.5 points)
vi) Hemoptysis - (1 point)
vii) Malignancy - (1 point)
A score of greater than 4 is considered "PE likely" whereas a score of 4 or less is considered "PE unlikely". A reasonable approach is to pursue CTA in the "PE likely" group and consider d-dimer (ELISA) testing in the "PE unlikely" group. One caveat is that most of these studies were done in outpatients and the approach of using d-dimer testing may not be generalizable to admitted GIM patients. Often this means going directly to CTA.
Remember, PIOPED II demonstrated that if the results of CTA are discordant with your clinical assessment (i.e. CTA negative in a high pre-test probability patient or positive in a low risk patient), this should promote additional testing.
2) After the diagnosis is made, anticoagulation should be initiated with heparin first (preferably LMWH over IV heparin) or Fondaparinux. The patient can then be bridged onto warfarin for a minimum of 3-6 months of anticoagulation. The exception to this is in patients with an active malignancy or receiving chemo where the CLOT Trial showed that anticoagulation with LMWH is superior to warfarin in preventing recurrent VTE and may reduce mortality in patients with solid tumors (sub-group analysis).
3) Consider thrombolysis in patients with hemodynamic instability from an acute PE.
4) The only indication for IVC filter insertion recommended in the 2008 ACCP Guidelines is for patients with a PE and a contraindication to anticoagulation. Furthermore, if an IVC filter is inserted, anticoagulation should be re-instituted as soon as is deemed safe.
5) Some authorities suggest inserting an IVC filter in the context of a recurrent pulmonary embolism while on anti-coagulation.
6) Controversy exists regarding the role of IVC filter placement in patients with poor cardiopulmonary reserve or a large clot burden.
7) "Prophylactic" IVC filters should be avoided.
8) The largest trials to date have shown that in hemodynamically stable patients, IVC filters reduce the incidence of recurrent symptomatic PEs, but do not change mortality and cause an increased rate of DVTs (when left in). The benefits may be greater in hemodynamically unstable patients.
9) Most IVC filters are retrievable! Talk to Interventional Radiology and arrange to have them removed. Do not leave your patient with a long term IVC filter unless they still need it!
No comments:
Post a Comment