
Today we discussed acute monoarthritis. Some points about the general approach and specific causes:
First question: Is this really arthritis (i.e. is it articular)? Important because non-articular causes are completely different (edema, ligamentous, tendon injury, etc)
Articular: Pain with any range of motion, effusion, morning stiffness, jt line tenderness. If multiple areas involved, more likely articular
Non-articular: Pain with specific ranges of motion, none of above.
Common causes of acute mono or pauciarthritis:
Septic arthritis- S. aureus, N. gonorrhea, S. pneumo
Crystal- gout/CPPD
Seronegative arthritis- esp. reactive, IBD-associated
RA (mono-articular)
Sarcoidosis (often bilateral ankle)
Trauma (fracture, hemarthrosis)
Common causes of acute polyarticular arthritis:
Endocarditis
Viral (HBV, HIV, parvo)
Serum sickness (drug rxn)
RA
SLE
Lyme (may also be monoarticular)
Some general features of specific causes:
Septic arthritis:
Risk factors: age, diabetes mellitus, rheumatoid arthritis, joint surgery, hip or knee prosthesis, skin infection, HIV, IV drug use
Clinical features: Joint pain in ~85%, joint welling in ~80%, and fever in ~60%
There are no physical exam findings that reliably rule in or out septic arthritis according JAMA Rational Clinical Exam paper linked below
Joint aspirate:
WBC over 100,000- Positive LR 28
WBC over 25,000- Positive LR 2.9
WBC less than 25,000- Negative LR 0.32
PMN over 90%- Positive LR 3.4; Negative LR 0.34
Also send for Gram stain, C+S, crystals
Common organisms:
St. aureus, St. pneumo, N. gonorrheae, Gram neg bacilli
Empiric tx: vancomycin and ceftriaxone
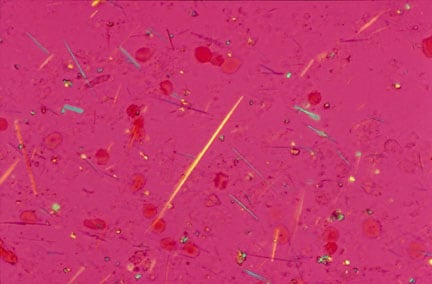
Crystal arthritis:
NB- finding crystals does not rule out septic joint! Can present the same way with fever, high WBC.
Gout vs pseudogout:
Gout: needle-like crystals, negatively birefringent, 1st MTP/ankle/knee. Risk factors are hyperuricemia, obesity, culprit meds (HCTZ, low dose ASA, others)
{kind=link}
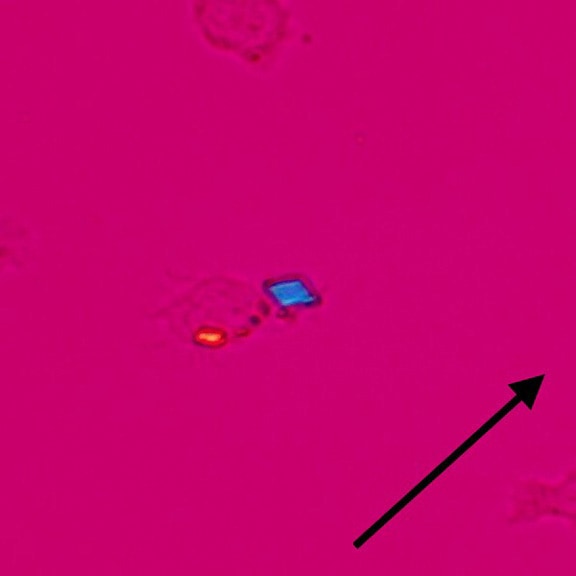
CPPD: rhomboid crystals inside macrophages, often hemorrhagic synovial fluid, positively birefringent. Knee, wrist, other. Risk factors: hypercalcemia, hemochromatosis, CKD.
{kind=link}
Gout therapy
Acutely: Options are NSAID/colchicine/intra-articular steroid/systemic steroid
NSAID: Not in CHF or renal failure
Colchicine: Works, but often limited by GI side effects
Steroid:
Intra-articular highly effective with 1-2 jts. Confirm the diagnosis first.
Systemic- Prednisone 30-50mg PO x 3-5d then stop. Works well, but side effects.
Chronically: if 3 or more attacks per years, consider allopurinol
Links:
Click here for CMAJ review of monoarthritis
Click here for JAMA: Does this Patient have Septic Arthritis?
Am Abdul Hakim so joyful giving this testimony of genius herbalist,Dr Moses anabic herbal home whom cured me of liver cancer.i was diagnosed of liver cancer 2years back I tried to cope with the sickness but unfortunately it had gone so bad,I went to so many medical centres I was told to go for a special xray which was computed tomography scan.it's result came out that my liver was rottening and was told that there was no cure,I collapsed there at the centre after getting myself an individual who came for a test after being cured from hiv,then gave me an email address of dr Moses anabic so I contacted him and he assured me of a total cure after three weeks of administering his herbs and I was cured totally.nothing is impossible for God almighty any individual suffering from any illness or virus no matter how bad it may be,don't ever think it's impossible.contact him through his personal email address via MOSESANABIC@GMAIL.COM or write him on WhatsApp with +2348100661264.thank you very much doctor Moses.
ReplyDelete